Tech Trends

Chinmay Chandgude
Healthcare Software Development Trends in 2026: What Product Teams Are Actually Building

The U.S. digital health market is valued at $106 billion in 2026 and projected to reach $266 billion by 2035, according to Precedence Research's Digital Health Market report. That number tells you where the money is. The trends below tell you where the product teams are.
Healthcare software in 2026 is not in a "figuring it out" phase. The experiments are over. Product teams are shipping AI documentation tools into production, rebuilding remote monitoring platforms around new CMS billing codes, and making FHIR the starting point of architecture, not an afterthought. The question is no longer whether to build these capabilities. It is whether your team has the architecture and compliance foundations to build them without breaking clinical workflows or creating regulatory exposure.
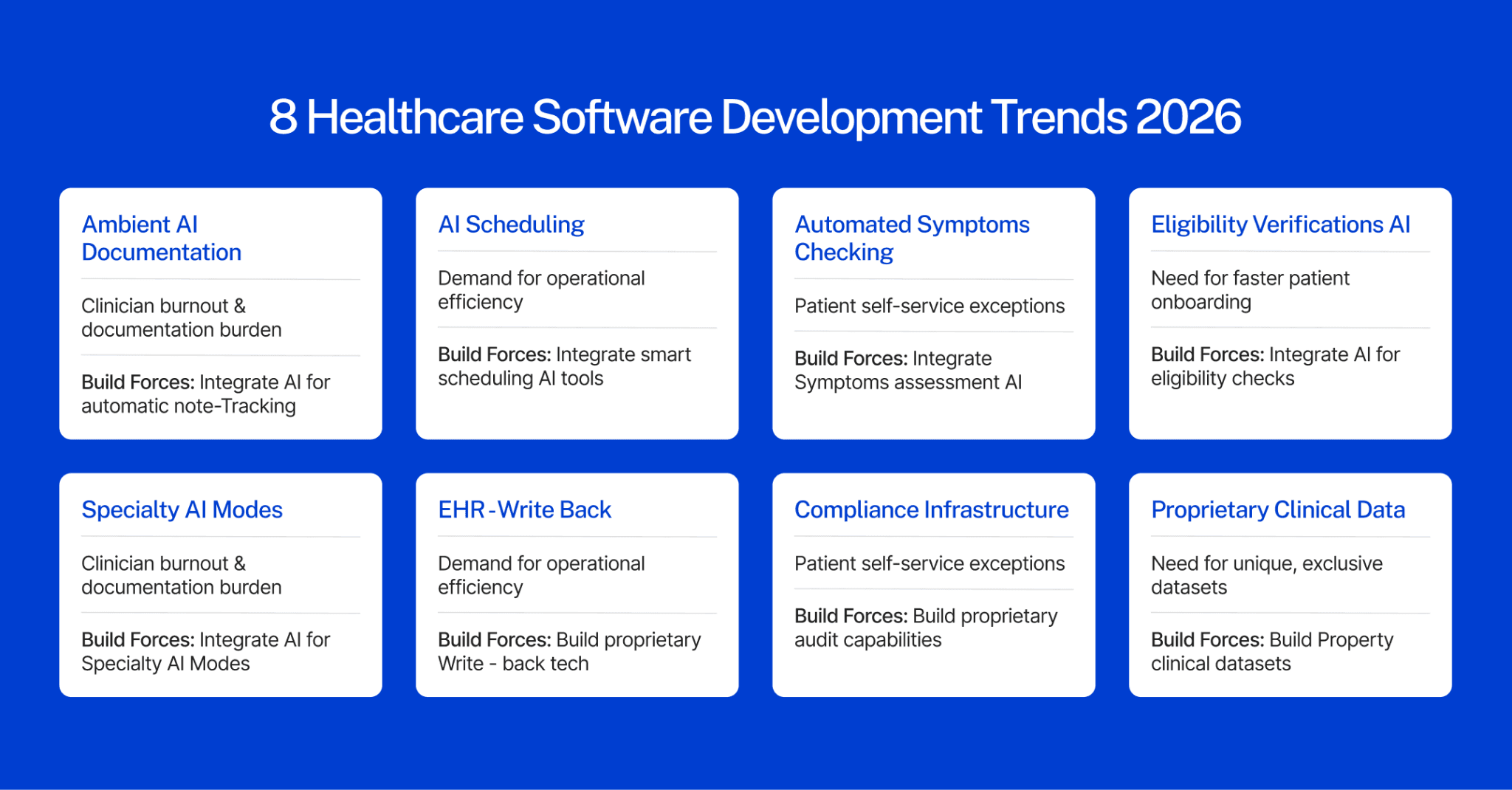
This guide covers the eight trends shaping what U.S. product teams are actually building right now with context on what each trend means for your technical decisions, your compliance posture, and your product roadmap.
1. Ambient AI Documentation Has Left the Pilot Phase
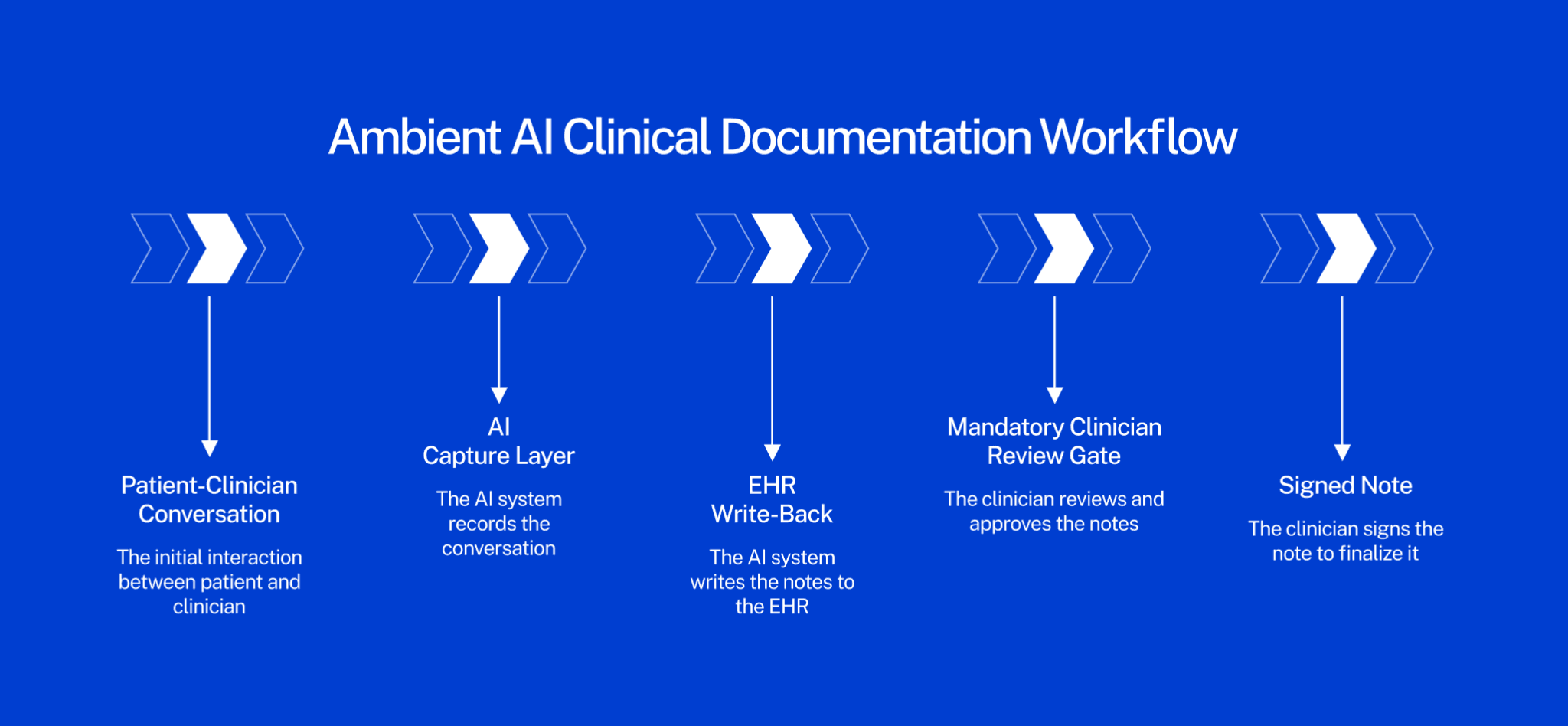
Ambient AI documentation where a clinical AI listens to a patient-provider conversation and generates structured clinical notes in real time has crossed from proof-of-concept to enterprise deployment at major U.S. health systems.
The ambient AI scribe market now includes more than 50 vendors, according to a 2026 medical practice revenue analysis by RevEleMD. Meditech, Epic, athenahealth, and Oracle Health have all deepened ambient AI integration into their core EHR workflows. Mass General Brigham made ambient documentation available to all its physicians by April 2025, with more than 3,000 providers routinely using the tools and the Emory and UW Health systems have published findings showing providers report measurably less burnout and lower after-hours documentation after adoption.
The pressure driving all of this is well-documented: clinicians are losing nearly 90 minutes per day to administrative tasks, according to symplr's fourth annual Compass Survey, covered by Managed Healthcare Executive. Ambient scribes reclaim that time. Early-adopter health systems also report more comprehensive diagnosis documentation per encounter, which directly improves revenue capture without upcoding.
What this means for your product build: Ambient AI is not a standalone feature. It requires deep EHR write-back integration, consent management infrastructure for audio recording including state wiretapping law compliance role-based access controls, and a mandatory clinician review layer. The liability surface area for documentation errors is substantial. "Automation bias," where a clinician signs an AI-generated note without reviewing it, creates both malpractice and False Claims Act exposure. If you are building ambient AI into a clinical product, the review mechanism is not optional; it is the compliance foundation the entire product rests on.
What teams are building in this space: EHR-integrated ambient documentation modules, specialty-tuned models for high-documentation settings such as primary care, psychiatry, and emergency medicine, audit trail systems tied to clinician sign-off events, and automated coding suggestion layers that sit downstream of clinical review.
Building an AI-powered clinical documentation tool? Our managed pod owns the EHR integration, compliance architecture, and HIPAA audit trail from sprint one, before you commit. Start your free discovery sprint →
2. Remote Patient Monitoring Is Now a Reimbursement Story
Remote patient monitoring was always clinically compelling. In 2026, it has finally become financially sustainable for providers to deploy at scale because the billing rules changed.
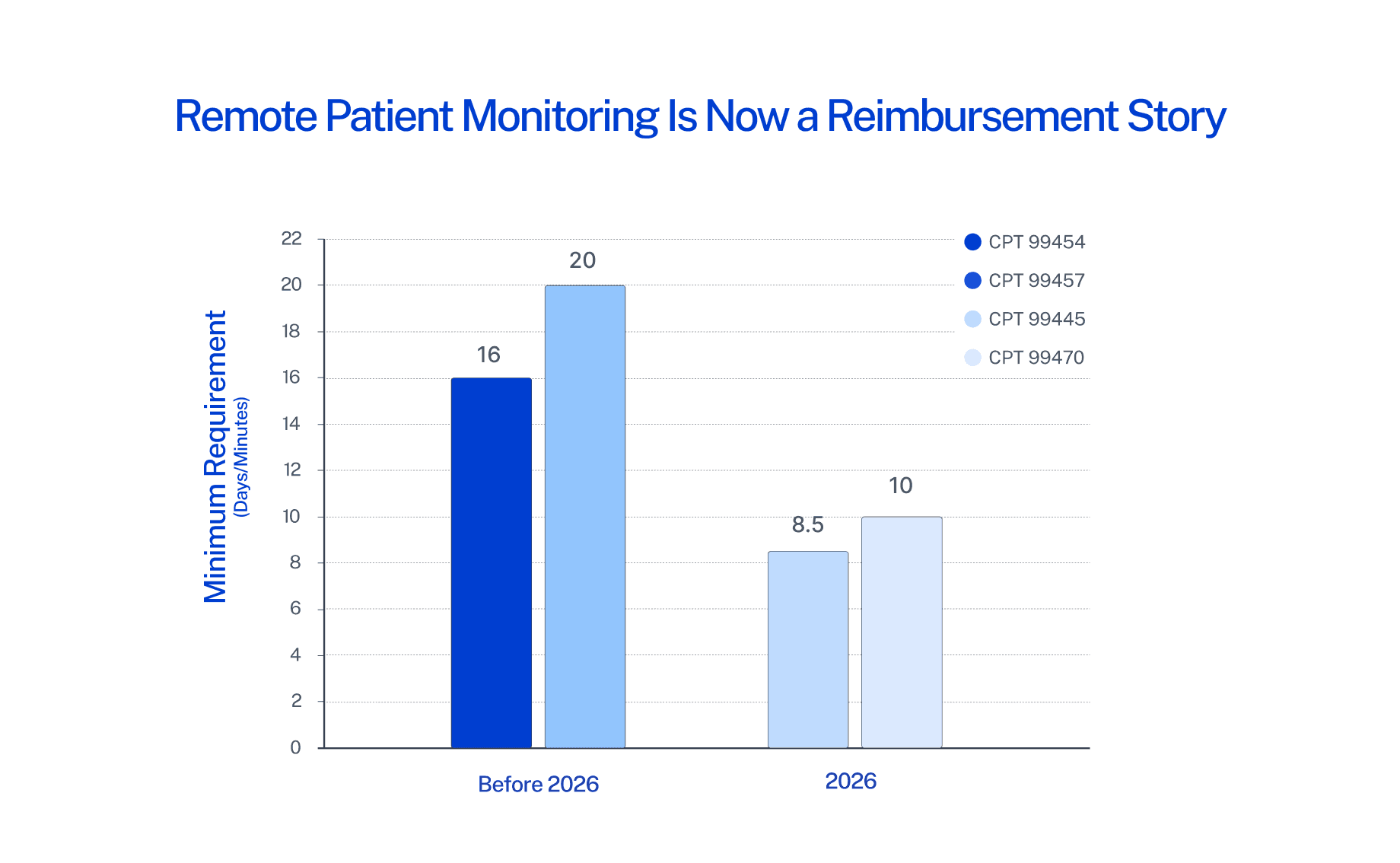
The CMS 2026 Physician Fee Schedule introduced two new RPM CPT codes: 99445 covers device supply for patients who transmit physiologic data on 2–15 days in a 30-day period (previously the only device supply code required 16 days minimum), and 99470 covers the first 10 minutes of treatment management services in a calendar month (previously required 20 minutes). Parallel updates were made for Remote Therapeutic Monitoring with new codes 98985 and 98979. All the details of these codes, requirements, reimbursement rates, and billing rules are covered in Tenovi's 2026 RPM CPT code guide.
These changes are not minor adjustments. They fundamentally expand which patient populations and care episodes qualify for RPM reimbursement including post-surgical recovery, medication titration periods, episodic care, and patients with inconsistent monitoring adherence who previously fell below billing thresholds. Providers can now build RPM programs around actual patient needs rather than around the billing minimums.
The market numbers reflect sustained momentum. The U.S. RPM market was valued at approximately $14.3 billion in 2024 and is projected to exceed $18 billion by 2026. An estimated 71 million Americans are expected to use RPM by 2025, roughly 26% of the population and Medicare RPM claims have grown more than 3,000% since 2019, according to OmniMD's RPM statistics and trends report.
What this means for your product build: The reimbursement change shifts the product priority list. Winning RPM platforms in 2026 are built for documentation accuracy and billing code compliance, not just device connectivity. If your platform cannot automatically generate documentation that satisfies CPT 99445 and 99470 requirements, providers cannot bill for the services delivered and they will not deploy your platform at scale.
What teams are building in this space: AI-prioritized alert management to cut clinical noise, automated documentation tied to CPT billing thresholds, EHR-integrated data pipelines for device data, short-episode monitoring workflows for post-discharge use cases, and patient-facing adherence tools to maintain minimum data transmission rates.
For teams building telehealth-integrated RPM tools, our guide on telemedicine platform development architecture covers the key technical decisions in detail.
3. FHIR-Native Architecture Is the Default Starting Point
A few years ago, FHIR was something product teams bolted on during integration. In 2026, it is how teams start.
The shift is driven by two forces working together. The 21st Century Cures Act's information blocking provisions have made FHIR compliance non-negotiable for any application that connects to clinical data. At the same time, the major EHR vendors — Epic, Oracle Health (formerly Cerner), athenahealth have all deepened their FHIR R4 API support, creating a practical ecosystem where FHIR-first architectures get faster integrations, cleaner compliance postures, and better interoperability with downstream analytics and AI tools.
Increased interoperability focus is one of the defining trends in healthcare IT investment in 2026, with health system CIOs treating data exchange capability as foundational infrastructure for every AI and analytics initiative they are building, according to Becker's Hospital Review's analysis of 2026 technology trends.
SMART on FHIR the OAuth 2.0-based authorization framework that governs how third-party apps authenticate with EHR systems is now a required technical competency for any team building healthcare applications that touch clinical data. It is no longer specialized knowledge. It is a baseline requirement for getting into the ecosystem.
What this means for your product build: Teams that start with a proprietary data model and add FHIR compatibility later consistently spend more time and money on rework than teams that design FHIR-first. This is an architecture decision that compounds: the longer you wait, the more expensive the retrofit becomes. Every sprint spent building on a non-FHIR data model is a sprint that may need to be partially undone.
What teams are building in this space: FHIR R4 and R4B compliant data models, SMART on FHIR app authorization flows, HL7 v2 translation layers for legacy EHR environments, patient data access APIs that satisfy ONC certification requirements, and FHIR-based care gap identification tools for value-based care programs.
For a deeper look at how EHR integration decisions affect product architecture, see our breakdown of top EMR integration tools and what healthcare product teams actually use.
4. AI-Augmented Clinical Decision Support Now Has a Formal Regulatory Structure
For the first time, AI assistance in clinical decision-making has a dedicated coding and billing framework in the United States.
The 2026 CPT code updates include seven new codes covering AI-augmented services across radiology, pathology, cardiology, and diagnostics. This is the first comprehensive incorporation of AI-augmented medical codes since the concept was introduced in 2022 and it matters because it creates the documentation, billing, and reimbursement infrastructure that makes AI-assisted clinical services financially sustainable for providers to deploy.
CMS also launched the WISeR (Wasteful and Inappropriate Service Reduction) model in January 2026, piloting AI-supported prior authorization for traditional Medicare in six states. This kind of federal-level AI integration into core reimbursement infrastructure signals the direction clearly: AI in clinical settings is moving from optional tooling to an embedded layer of care delivery that has formal regulatory recognition.
What this means for your product build: AI decision support features are regulated clinical features in 2026, not software features. That distinction matters for how you build. It means building explainability into model outputs, integrating mandatory clinician review requirements into the product workflow, and designing audit trail infrastructure that can withstand a compliance review tied to CPT documentation requirements. Teams that treat AI decision support as a software module rather than a regulated clinical capability will face enforcement and liability exposure as the framework matures.
What teams are building in this space: AI-assisted diagnostic tools with explainability layers designed for the new CPT audit requirements, cardiology and radiology workflow integration, predictive risk models with clinician-facing output formats, prior authorization automation tools aligned with the WISeR model, and audit databases designed for CPT documentation compliance.
5. Mental Health and Behavioral Health Software Is Its Own Category
Mental health software used to be treated as a subset of general wellness applications. In 2026, it is a standalone development category with its own compliance stack, distinct feature requirements, and a user population that demands careful product design.
The growth data is significant: the mental health and behavioral health segment is projected to be the fastest-growing disease category in digital health from 2025 to 2030, according to MarketsandMarkets' digital health market forecast. The regulatory complexity sits on top of that growth: HIPAA applies broadly, but 42 CFR Part 2 governs substance use disorder records with stricter consent requirements than standard clinical data, and many states have added mental health privacy protections that exceed federal minimums. California, New York, and several other states have enacted laws that treat mental health data more restrictively than HIPAA requires.
The product design challenge is equally specific. Safe messaging guidelines developed by organizations like AFSP and SAMHSA dictate how mental health apps must handle crisis content, suicidal ideation references, and escalation pathways. A wellness app that does not account for these guidelines creates both clinical risk and regulatory exposure. Telehealth mental health visits have normalized across age groups, employer-sponsored mental health benefits are expanding, and the patient population now spans adolescents to seniors — each with different UX and compliance requirements.
What this means for your product build: You cannot build a compliant mental health product by adding a HIPAA checkbox to a general wellness app. The compliance surface includes 42 CFR Part 2 consent workflows, state-specific mental health privacy laws, safe messaging guideline compliance in all patient-facing content, crisis escalation routing with warm handoff capabilities, and session note confidentiality controls that differ from standard clinical documentation. These are architecture requirements, not feature additions. They need to be designed in from day one.
What teams are building in this space: Behavioral health-specific EHR modules with 42 CFR Part 2 consent workflows, crisis escalation and routing tools, therapist-facing documentation with specialty-specific note templates, employer-sponsored mental health benefit platforms, and asynchronous care tools for patient-therapist communication between scheduled sessions.
Our post on key requirements for building mental health software covers the full compliance specification and feature requirements in detail.
6. Legacy System Modernization Is Finally Getting Budget
Healthcare has known about its legacy system problem for decades. In 2026, a combination of interoperability mandates, cybersecurity pressure, and AI adoption prerequisites is forcing organizations to fund the work.
Over 85% of healthcare organizations now operate on cloud-based EHRs, yet many still carry on-premise legacy systems running in parallel, creating data fragmentation, security exposure, and integration bottlenecks, according to Ulam's 2026 healthtech software trends analysis. That same analysis notes that 2024 saw a 15% increase in healthcare data breaches, with several of the most damaging incidents tracing directly to outdated systems with inadequate security architecture. The breach environment has generated board-level pressure that efficiency arguments alone never produced.
The AI integration argument is pushing the same direction: ambient documentation tools, FHIR-native data exchange, and real-time RPM analytics simply cannot be integrated with systems that predate modern API architecture. Legacy modernization has become a prerequisite for every other trend on this list.
Health system CIOs are responding by scrutinizing technology investments more carefully in 2026 — not by investing less, but by demanding that investments deliver cohesive, enterprise-wide value rather than adding more point-solution complexity to an already fragmented stack, according to Becker's Hospital Review's 2026 CIO technology investment analysis.
What this means for your product build: Legacy modernization creates two distinct product opportunities. The first is migration tooling — data extraction, transformation, and validation tools that move clinical data from legacy formats into modern schemas without breaking clinical continuity. The second is integration middleware — layers that allow legacy systems to communicate with modern applications without requiring a full replacement, buying time while the longer migration plays out. Both have strong commercial demand from health systems facing the same pressure from multiple directions simultaneously.
What teams are building in this space: HL7 v2 to FHIR R4 conversion services, modular EHR replacement components designed to replace legacy modules rather than entire systems, data migration validation tools with clinical data integrity checks, API gateways that expose legacy data in FHIR format for downstream applications, and cloud migration infrastructure for on-premise clinical systems.
7. Patient Engagement Software Is Being Rebuilt Around Behavior Change
The first generation of patient engagement software optimized for features appointment reminders, portal access, care plan delivery. In 2026, the second generation is optimizing for behavior change.
The reason for the shift is adoption data. Over 85% of healthcare organizations operate on cloud-based EHRs, yet patient portal adoption rates remain well below what providers expected when they deployed those systems. The issue is that these tools were built around information delivery, the assumption that giving patients access to information changes what they do. The evidence from behavioral economics says otherwise, and product teams are building accordingly.
The 2026 Best in KLAS report added a new "Patient Engagement: Other Validated Software" category for the first time, reflecting the segment's maturation into a distinct evaluation category in healthcare IT procurement. When KLAS creates a new category, it signals that buyers are purchasing these tools at a scale that warrants a dedicated performance benchmark — the market has arrived.
Product teams in 2026 are building with different assumptions: personalization engines that adapt communication timing, frequency, and channel to individual patient preferences; conversational AI interfaces that reduce friction in clinical communication; asynchronous messaging tools that give patients a lower-stakes way to engage with their care team between appointments; and habit-loop design frameworks for chronic disease management apps where sustained behavior change is the actual clinical outcome.
What this means for your product build: The design constraint in this category is building for patients who are not already motivated. Building for engaged, health-literate users is not the challenge. Building for patients who are overwhelmed, time-constrained, or skeptical of digital health tools is where the real product work happens and it requires behavioral design expertise that clinical product teams typically do not have in-house.
What teams are building in this space: Personalized multi-channel communication engines with individual preference learning, conversational AI patient interfaces for appointment scheduling and care navigation, chronic disease management apps built on habit-loop design principles, asynchronous secure messaging platforms, and care gap closure tools tied to payer performance metrics and value-based care contracts.
8. Cybersecurity Is a Product Architecture Decision in 2026
Healthcare cybersecurity in 2026 has moved from the compliance team's problem to the product team's problem. The attack surface expands with every new connection: more APIs, more third-party integrations, more ambient sensors, more mobile access points, more cloud services. The perimeter has dissolved, and security architecture decisions made at the product level determine what exposure the organization carries.
The breach environment reinforces this. In 2024, healthcare saw a 15% increase in data breaches, with the most damaging incidents tracing to inadequate security architecture in legacy and connected systems, noted by Ulam's 2026 healthtech analysis. Health system CIOs have elevated cybersecurity as a 2026 investment priority, with a specific focus on ensuring security investments produce cohesive control environments rather than layers of disconnected point solutions, according to Becker's Hospital Review's 2026 CIO technology investment analysis.
The 2026 Best in KLAS rankings added a new "Cybersecurity Solutions" category alongside a new "Patient Engagement: Other Validated Software" category, signaling that cybersecurity capability is now evaluated as a standalone product attribute in healthcare IT procurement decisions — not just a compliance checkbox vendors can self-certify.
What this means for your product build: Security architecture decisions made during the design phase cost a fraction of what remediations cost after deployment. Zero-trust architecture, role-based access control designed to clinical workflow specifications, end-to-end encryption as default, and audit logging built into the data model are design decisions — not IT decisions that get added later. Products that cannot produce detailed security architecture documentation in an enterprise procurement process will lose evaluations to products that can. This is happening right now in RFPs across major U.S. health systems.
What teams are building in this space: Zero-trust API architecture for connected healthcare platforms, role-based access control systems with clinical workflow awareness, end-to-end encryption with structured key management documentation, audit trail databases designed for HIPAA enforcement review, and automated security scanning integrated into the CI/CD pipeline.
The Pattern Across All Eight Trends
Every trend above shares a through-line: the work that separates product teams that ship from teams that stall is not the technology choice, it is the architecture and compliance foundation those choices are built on.
The ambient AI vendor that does not understand documentation liability builds a product that creates legal risk. The RPM platform that does not account for 2026 CPT requirements builds a product providers cannot bill for. The team that treats FHIR as an afterthought spends six months undoing architecture decisions made in the first sprint. The cybersecurity-light product fails the enterprise procurement evaluation before it reaches a clinical decision-maker.
Healthcare software in 2026 rewards teams that start with compliance, workflow, and integration architecture before writing the first line of code. That sequence - design for compliance first, then features, is the pattern that is working across every category on this list.
Summary: 8 Healthcare Software Development Trends in 2026
Trend | What's Driving It | What Teams Are Building |
Ambient AI Documentation | 50+ vendors, enterprise deployment at major U.S. health systems | EHR write-back integration, consent workflows, clinician review gates, audit trails |
RPM Reimbursement Changes | New 2026 CMS CPT codes 99445 & 99470 | Billing-compliant documentation automation, short-episode monitoring workflows |
FHIR-Native Architecture | 21st Century Cures Act, Epic/Oracle/athenahealth API deepening | FHIR R4 data models, SMART on FHIR authorization flows |
AI Clinical Decision Support | 7 new CPT codes for AI-augmented services, WISeR prior auth model | Explainability layers, CPT-compliant audit trails, prior auth automation |
Mental/Behavioral Health Software | 42 CFR Part 2, fastest-growing digital health segment 2025–2030 | Crisis escalation tools, specialty EHR modules, 42 CFR compliant consent flows |
Legacy Modernization | 15% breach increase in 2024, AI and FHIR prerequisites | HL7-to-FHIR conversion, integration middleware, cloud migration infrastructure |
Patient Engagement | New KLAS category, behavior change over information delivery | Personalization engines, conversational AI, habit-loop design for chronic disease |
Cybersecurity Architecture | New KLAS cybersecurity category, breach growth, CIO scrutiny | Zero-trust APIs, role-based access control, HIPAA audit trail databases |
Where to Go From Here
Eight trends. One common thread: healthcare software in 2026 punishes teams that treat compliance, interoperability, and security as later-stage problems. The teams making progress shipping ambient AI tools that don't create liability, building RPM platforms that providers can actually bill for, passing enterprise security evaluations without scrambling are the ones that resolved those questions in the architecture phase, before product development started.
If you're in the middle of scoping a healthcare product or trying to figure out whether your current architecture will hold up to what's ahead, that's exactly the conversation our team is built for. We have shipped more than 100 healthcare products across EMR, telehealth, medical device, and wellness categories and every engagement starts before you commit, with an architecture review, a product scope, and a team design delivered in the first two weeks.
If any of the trends above are relevant to what you're building, book a free 30-minute call with us. No pitch, no obligation, just a direct conversation about your product, your architecture questions, and whether we're the right fit to help you build it.
Frequently Asked Questions
What are the top healthcare software development trends in 2026?
The eight leading trends are: ambient AI documentation moving to enterprise production, new CMS reimbursement codes making remote patient monitoring financially scalable, FHIR-native architecture as the default starting point for EHR-connected applications, a formal CPT billing structure for AI-augmented clinical decision support, behavioral health software as a standalone regulated category, legacy system modernization driven by cybersecurity and AI prerequisites, patient engagement software rebuilt around behavioral economics rather than information delivery, and cybersecurity treated as product architecture from day one. Each reflects the shift from piloting technologies to shipping production-grade systems with compliance and integration requirements built in from the start.
How is AI changing healthcare software development for U.S. product teams in 2026?
AI in 2026 has three primary application areas for U.S. product teams: ambient documentation integrated directly into clinical EHR workflows, clinical decision support tools backed by new CPT billing codes that enable formal reimbursement for AI-assisted services, and revenue cycle automation covering prior authorization, denial management, and claims optimization. CMS's January 2026 launch of the WISeR model — AI-supported prior authorization piloted in six states — signals the regulatory direction. Product teams are building explainability layers, audit trails, and mandatory clinician review workflows into AI features to manage the liability and compliance surface that clinical AI creates.
Why does FHIR matter for healthcare software product teams in 2026?
FHIR (Fast Healthcare Interoperability Resources) is the federal standard governing clinical data exchange, mandated by the 21st Century Cures Act's information blocking provisions. Any application connecting to major EHR platforms like Epic, Oracle Health, or athenahealth must be FHIR R4 compliant to participate in those ecosystems. SMART on FHIR is the specific OAuth 2.0 authorization framework those platforms use to authenticate third-party apps. Product teams that build FHIR-native from the architecture phase avoid significant rework, integration delays, and compliance gaps compared to teams that attempt to retrofit FHIR compatibility into an existing proprietary data model.
What did CMS change about remote patient monitoring reimbursement in 2026?
CMS's 2026 Physician Fee Schedule introduced CPT code 99445, which covers RPM device supply for patients who transmit physiologic data on 2–15 days in a 30-day period — previously, the only device supply code required a 16-day minimum. It also introduced CPT code 99470, which covers the first 10 minutes of treatment management services per month, down from the 20-minute minimum previously required under CPT 99457. These changes expand RPM eligibility to post-surgical recovery, episodic care, and patients with inconsistent monitoring adherence who were not reimbursable under prior rules, making RPM viable for a significantly larger patient population.
What does building a HIPAA-compliant healthcare app in 2026 actually require?
HIPAA technical safeguards in 2026 require zero-trust architecture across API connections, clinically aware role-based access controls, end-to-end encryption with documented key management, audit logging built into the data model (not added as an afterthought), documented patient consent workflows, and fully executed Business Associate Agreements with every third-party integration. Enterprise health system buyers now conduct detailed security architecture reviews before vendor selection, asking specifically how encryption, access control, and audit logging are implemented, not just whether a vendor claims HIPAA compliance. Security architecture documentation needs to be production-ready before the enterprise sales process begins.
The U.S. digital health market is valued at $106 billion in 2026 and projected to reach $266 billion by 2035, according to Precedence Research's Digital Health Market report. That number tells you where the money is. The trends below tell you where the product teams are.
Healthcare software in 2026 is not in a "figuring it out" phase. The experiments are over. Product teams are shipping AI documentation tools into production, rebuilding remote monitoring platforms around new CMS billing codes, and making FHIR the starting point of architecture, not an afterthought. The question is no longer whether to build these capabilities. It is whether your team has the architecture and compliance foundations to build them without breaking clinical workflows or creating regulatory exposure.
This guide covers the eight trends shaping what U.S. product teams are actually building right now with context on what each trend means for your technical decisions, your compliance posture, and your product roadmap.
1. Ambient AI Documentation Has Left the Pilot Phase
Ambient AI documentation where a clinical AI listens to a patient-provider conversation and generates structured clinical notes in real time has crossed from proof-of-concept to enterprise deployment at major U.S. health systems.
The ambient AI scribe market now includes more than 50 vendors, according to a 2026 medical practice revenue analysis by RevEleMD. Meditech, Epic, athenahealth, and Oracle Health have all deepened ambient AI integration into their core EHR workflows. Mass General Brigham made ambient documentation available to all its physicians by April 2025, with more than 3,000 providers routinely using the tools and the Emory and UW Health systems have published findings showing providers report measurably less burnout and lower after-hours documentation after adoption.
The pressure driving all of this is well-documented: clinicians are losing nearly 90 minutes per day to administrative tasks, according to symplr's fourth annual Compass Survey, covered by Managed Healthcare Executive. Ambient scribes reclaim that time. Early-adopter health systems also report more comprehensive diagnosis documentation per encounter, which directly improves revenue capture without upcoding.
What this means for your product build: Ambient AI is not a standalone feature. It requires deep EHR write-back integration, consent management infrastructure for audio recording including state wiretapping law compliance role-based access controls, and a mandatory clinician review layer. The liability surface area for documentation errors is substantial. "Automation bias," where a clinician signs an AI-generated note without reviewing it, creates both malpractice and False Claims Act exposure. If you are building ambient AI into a clinical product, the review mechanism is not optional; it is the compliance foundation the entire product rests on.
What teams are building in this space: EHR-integrated ambient documentation modules, specialty-tuned models for high-documentation settings such as primary care, psychiatry, and emergency medicine, audit trail systems tied to clinician sign-off events, and automated coding suggestion layers that sit downstream of clinical review.
Building an AI-powered clinical documentation tool? Our managed pod owns the EHR integration, compliance architecture, and HIPAA audit trail from sprint one, before you commit. Start your free discovery sprint →
2. Remote Patient Monitoring Is Now a Reimbursement Story
Remote patient monitoring was always clinically compelling. In 2026, it has finally become financially sustainable for providers to deploy at scale because the billing rules changed.
The CMS 2026 Physician Fee Schedule introduced two new RPM CPT codes: 99445 covers device supply for patients who transmit physiologic data on 2–15 days in a 30-day period (previously the only device supply code required 16 days minimum), and 99470 covers the first 10 minutes of treatment management services in a calendar month (previously required 20 minutes). Parallel updates were made for Remote Therapeutic Monitoring with new codes 98985 and 98979. All the details of these codes, requirements, reimbursement rates, and billing rules are covered in Tenovi's 2026 RPM CPT code guide.
These changes are not minor adjustments. They fundamentally expand which patient populations and care episodes qualify for RPM reimbursement including post-surgical recovery, medication titration periods, episodic care, and patients with inconsistent monitoring adherence who previously fell below billing thresholds. Providers can now build RPM programs around actual patient needs rather than around the billing minimums.
The market numbers reflect sustained momentum. The U.S. RPM market was valued at approximately $14.3 billion in 2024 and is projected to exceed $18 billion by 2026. An estimated 71 million Americans are expected to use RPM by 2025, roughly 26% of the population and Medicare RPM claims have grown more than 3,000% since 2019, according to OmniMD's RPM statistics and trends report.
What this means for your product build: The reimbursement change shifts the product priority list. Winning RPM platforms in 2026 are built for documentation accuracy and billing code compliance, not just device connectivity. If your platform cannot automatically generate documentation that satisfies CPT 99445 and 99470 requirements, providers cannot bill for the services delivered and they will not deploy your platform at scale.
What teams are building in this space: AI-prioritized alert management to cut clinical noise, automated documentation tied to CPT billing thresholds, EHR-integrated data pipelines for device data, short-episode monitoring workflows for post-discharge use cases, and patient-facing adherence tools to maintain minimum data transmission rates.
For teams building telehealth-integrated RPM tools, our guide on telemedicine platform development architecture covers the key technical decisions in detail.
3. FHIR-Native Architecture Is the Default Starting Point
A few years ago, FHIR was something product teams bolted on during integration. In 2026, it is how teams start.
The shift is driven by two forces working together. The 21st Century Cures Act's information blocking provisions have made FHIR compliance non-negotiable for any application that connects to clinical data. At the same time, the major EHR vendors — Epic, Oracle Health (formerly Cerner), athenahealth have all deepened their FHIR R4 API support, creating a practical ecosystem where FHIR-first architectures get faster integrations, cleaner compliance postures, and better interoperability with downstream analytics and AI tools.
Increased interoperability focus is one of the defining trends in healthcare IT investment in 2026, with health system CIOs treating data exchange capability as foundational infrastructure for every AI and analytics initiative they are building, according to Becker's Hospital Review's analysis of 2026 technology trends.
SMART on FHIR the OAuth 2.0-based authorization framework that governs how third-party apps authenticate with EHR systems is now a required technical competency for any team building healthcare applications that touch clinical data. It is no longer specialized knowledge. It is a baseline requirement for getting into the ecosystem.
What this means for your product build: Teams that start with a proprietary data model and add FHIR compatibility later consistently spend more time and money on rework than teams that design FHIR-first. This is an architecture decision that compounds: the longer you wait, the more expensive the retrofit becomes. Every sprint spent building on a non-FHIR data model is a sprint that may need to be partially undone.
What teams are building in this space: FHIR R4 and R4B compliant data models, SMART on FHIR app authorization flows, HL7 v2 translation layers for legacy EHR environments, patient data access APIs that satisfy ONC certification requirements, and FHIR-based care gap identification tools for value-based care programs.
For a deeper look at how EHR integration decisions affect product architecture, see our breakdown of top EMR integration tools and what healthcare product teams actually use.
4. AI-Augmented Clinical Decision Support Now Has a Formal Regulatory Structure
For the first time, AI assistance in clinical decision-making has a dedicated coding and billing framework in the United States.
The 2026 CPT code updates include seven new codes covering AI-augmented services across radiology, pathology, cardiology, and diagnostics. This is the first comprehensive incorporation of AI-augmented medical codes since the concept was introduced in 2022 and it matters because it creates the documentation, billing, and reimbursement infrastructure that makes AI-assisted clinical services financially sustainable for providers to deploy.
CMS also launched the WISeR (Wasteful and Inappropriate Service Reduction) model in January 2026, piloting AI-supported prior authorization for traditional Medicare in six states. This kind of federal-level AI integration into core reimbursement infrastructure signals the direction clearly: AI in clinical settings is moving from optional tooling to an embedded layer of care delivery that has formal regulatory recognition.
What this means for your product build: AI decision support features are regulated clinical features in 2026, not software features. That distinction matters for how you build. It means building explainability into model outputs, integrating mandatory clinician review requirements into the product workflow, and designing audit trail infrastructure that can withstand a compliance review tied to CPT documentation requirements. Teams that treat AI decision support as a software module rather than a regulated clinical capability will face enforcement and liability exposure as the framework matures.
What teams are building in this space: AI-assisted diagnostic tools with explainability layers designed for the new CPT audit requirements, cardiology and radiology workflow integration, predictive risk models with clinician-facing output formats, prior authorization automation tools aligned with the WISeR model, and audit databases designed for CPT documentation compliance.
5. Mental Health and Behavioral Health Software Is Its Own Category
Mental health software used to be treated as a subset of general wellness applications. In 2026, it is a standalone development category with its own compliance stack, distinct feature requirements, and a user population that demands careful product design.
The growth data is significant: the mental health and behavioral health segment is projected to be the fastest-growing disease category in digital health from 2025 to 2030, according to MarketsandMarkets' digital health market forecast. The regulatory complexity sits on top of that growth: HIPAA applies broadly, but 42 CFR Part 2 governs substance use disorder records with stricter consent requirements than standard clinical data, and many states have added mental health privacy protections that exceed federal minimums. California, New York, and several other states have enacted laws that treat mental health data more restrictively than HIPAA requires.
The product design challenge is equally specific. Safe messaging guidelines developed by organizations like AFSP and SAMHSA dictate how mental health apps must handle crisis content, suicidal ideation references, and escalation pathways. A wellness app that does not account for these guidelines creates both clinical risk and regulatory exposure. Telehealth mental health visits have normalized across age groups, employer-sponsored mental health benefits are expanding, and the patient population now spans adolescents to seniors — each with different UX and compliance requirements.
What this means for your product build: You cannot build a compliant mental health product by adding a HIPAA checkbox to a general wellness app. The compliance surface includes 42 CFR Part 2 consent workflows, state-specific mental health privacy laws, safe messaging guideline compliance in all patient-facing content, crisis escalation routing with warm handoff capabilities, and session note confidentiality controls that differ from standard clinical documentation. These are architecture requirements, not feature additions. They need to be designed in from day one.
What teams are building in this space: Behavioral health-specific EHR modules with 42 CFR Part 2 consent workflows, crisis escalation and routing tools, therapist-facing documentation with specialty-specific note templates, employer-sponsored mental health benefit platforms, and asynchronous care tools for patient-therapist communication between scheduled sessions.
Our post on key requirements for building mental health software covers the full compliance specification and feature requirements in detail.
6. Legacy System Modernization Is Finally Getting Budget
Healthcare has known about its legacy system problem for decades. In 2026, a combination of interoperability mandates, cybersecurity pressure, and AI adoption prerequisites is forcing organizations to fund the work.
Over 85% of healthcare organizations now operate on cloud-based EHRs, yet many still carry on-premise legacy systems running in parallel, creating data fragmentation, security exposure, and integration bottlenecks, according to Ulam's 2026 healthtech software trends analysis. That same analysis notes that 2024 saw a 15% increase in healthcare data breaches, with several of the most damaging incidents tracing directly to outdated systems with inadequate security architecture. The breach environment has generated board-level pressure that efficiency arguments alone never produced.
The AI integration argument is pushing the same direction: ambient documentation tools, FHIR-native data exchange, and real-time RPM analytics simply cannot be integrated with systems that predate modern API architecture. Legacy modernization has become a prerequisite for every other trend on this list.
Health system CIOs are responding by scrutinizing technology investments more carefully in 2026 — not by investing less, but by demanding that investments deliver cohesive, enterprise-wide value rather than adding more point-solution complexity to an already fragmented stack, according to Becker's Hospital Review's 2026 CIO technology investment analysis.
What this means for your product build: Legacy modernization creates two distinct product opportunities. The first is migration tooling — data extraction, transformation, and validation tools that move clinical data from legacy formats into modern schemas without breaking clinical continuity. The second is integration middleware — layers that allow legacy systems to communicate with modern applications without requiring a full replacement, buying time while the longer migration plays out. Both have strong commercial demand from health systems facing the same pressure from multiple directions simultaneously.
What teams are building in this space: HL7 v2 to FHIR R4 conversion services, modular EHR replacement components designed to replace legacy modules rather than entire systems, data migration validation tools with clinical data integrity checks, API gateways that expose legacy data in FHIR format for downstream applications, and cloud migration infrastructure for on-premise clinical systems.
7. Patient Engagement Software Is Being Rebuilt Around Behavior Change
The first generation of patient engagement software optimized for features appointment reminders, portal access, care plan delivery. In 2026, the second generation is optimizing for behavior change.
The reason for the shift is adoption data. Over 85% of healthcare organizations operate on cloud-based EHRs, yet patient portal adoption rates remain well below what providers expected when they deployed those systems. The issue is that these tools were built around information delivery, the assumption that giving patients access to information changes what they do. The evidence from behavioral economics says otherwise, and product teams are building accordingly.
The 2026 Best in KLAS report added a new "Patient Engagement: Other Validated Software" category for the first time, reflecting the segment's maturation into a distinct evaluation category in healthcare IT procurement. When KLAS creates a new category, it signals that buyers are purchasing these tools at a scale that warrants a dedicated performance benchmark — the market has arrived.
Product teams in 2026 are building with different assumptions: personalization engines that adapt communication timing, frequency, and channel to individual patient preferences; conversational AI interfaces that reduce friction in clinical communication; asynchronous messaging tools that give patients a lower-stakes way to engage with their care team between appointments; and habit-loop design frameworks for chronic disease management apps where sustained behavior change is the actual clinical outcome.
What this means for your product build: The design constraint in this category is building for patients who are not already motivated. Building for engaged, health-literate users is not the challenge. Building for patients who are overwhelmed, time-constrained, or skeptical of digital health tools is where the real product work happens and it requires behavioral design expertise that clinical product teams typically do not have in-house.
What teams are building in this space: Personalized multi-channel communication engines with individual preference learning, conversational AI patient interfaces for appointment scheduling and care navigation, chronic disease management apps built on habit-loop design principles, asynchronous secure messaging platforms, and care gap closure tools tied to payer performance metrics and value-based care contracts.
8. Cybersecurity Is a Product Architecture Decision in 2026
Healthcare cybersecurity in 2026 has moved from the compliance team's problem to the product team's problem. The attack surface expands with every new connection: more APIs, more third-party integrations, more ambient sensors, more mobile access points, more cloud services. The perimeter has dissolved, and security architecture decisions made at the product level determine what exposure the organization carries.
The breach environment reinforces this. In 2024, healthcare saw a 15% increase in data breaches, with the most damaging incidents tracing to inadequate security architecture in legacy and connected systems, noted by Ulam's 2026 healthtech analysis. Health system CIOs have elevated cybersecurity as a 2026 investment priority, with a specific focus on ensuring security investments produce cohesive control environments rather than layers of disconnected point solutions, according to Becker's Hospital Review's 2026 CIO technology investment analysis.
The 2026 Best in KLAS rankings added a new "Cybersecurity Solutions" category alongside a new "Patient Engagement: Other Validated Software" category, signaling that cybersecurity capability is now evaluated as a standalone product attribute in healthcare IT procurement decisions — not just a compliance checkbox vendors can self-certify.
What this means for your product build: Security architecture decisions made during the design phase cost a fraction of what remediations cost after deployment. Zero-trust architecture, role-based access control designed to clinical workflow specifications, end-to-end encryption as default, and audit logging built into the data model are design decisions — not IT decisions that get added later. Products that cannot produce detailed security architecture documentation in an enterprise procurement process will lose evaluations to products that can. This is happening right now in RFPs across major U.S. health systems.
What teams are building in this space: Zero-trust API architecture for connected healthcare platforms, role-based access control systems with clinical workflow awareness, end-to-end encryption with structured key management documentation, audit trail databases designed for HIPAA enforcement review, and automated security scanning integrated into the CI/CD pipeline.
The Pattern Across All Eight Trends
Every trend above shares a through-line: the work that separates product teams that ship from teams that stall is not the technology choice, it is the architecture and compliance foundation those choices are built on.
The ambient AI vendor that does not understand documentation liability builds a product that creates legal risk. The RPM platform that does not account for 2026 CPT requirements builds a product providers cannot bill for. The team that treats FHIR as an afterthought spends six months undoing architecture decisions made in the first sprint. The cybersecurity-light product fails the enterprise procurement evaluation before it reaches a clinical decision-maker.
Healthcare software in 2026 rewards teams that start with compliance, workflow, and integration architecture before writing the first line of code. That sequence - design for compliance first, then features, is the pattern that is working across every category on this list.
Summary: 8 Healthcare Software Development Trends in 2026
Trend | What's Driving It | What Teams Are Building |
Ambient AI Documentation | 50+ vendors, enterprise deployment at major U.S. health systems | EHR write-back integration, consent workflows, clinician review gates, audit trails |
RPM Reimbursement Changes | New 2026 CMS CPT codes 99445 & 99470 | Billing-compliant documentation automation, short-episode monitoring workflows |
FHIR-Native Architecture | 21st Century Cures Act, Epic/Oracle/athenahealth API deepening | FHIR R4 data models, SMART on FHIR authorization flows |
AI Clinical Decision Support | 7 new CPT codes for AI-augmented services, WISeR prior auth model | Explainability layers, CPT-compliant audit trails, prior auth automation |
Mental/Behavioral Health Software | 42 CFR Part 2, fastest-growing digital health segment 2025–2030 | Crisis escalation tools, specialty EHR modules, 42 CFR compliant consent flows |
Legacy Modernization | 15% breach increase in 2024, AI and FHIR prerequisites | HL7-to-FHIR conversion, integration middleware, cloud migration infrastructure |
Patient Engagement | New KLAS category, behavior change over information delivery | Personalization engines, conversational AI, habit-loop design for chronic disease |
Cybersecurity Architecture | New KLAS cybersecurity category, breach growth, CIO scrutiny | Zero-trust APIs, role-based access control, HIPAA audit trail databases |
Where to Go From Here
Eight trends. One common thread: healthcare software in 2026 punishes teams that treat compliance, interoperability, and security as later-stage problems. The teams making progress shipping ambient AI tools that don't create liability, building RPM platforms that providers can actually bill for, passing enterprise security evaluations without scrambling are the ones that resolved those questions in the architecture phase, before product development started.
If you're in the middle of scoping a healthcare product or trying to figure out whether your current architecture will hold up to what's ahead, that's exactly the conversation our team is built for. We have shipped more than 100 healthcare products across EMR, telehealth, medical device, and wellness categories and every engagement starts before you commit, with an architecture review, a product scope, and a team design delivered in the first two weeks.
If any of the trends above are relevant to what you're building, book a free 30-minute call with us. No pitch, no obligation, just a direct conversation about your product, your architecture questions, and whether we're the right fit to help you build it.
Frequently Asked Questions
What are the top healthcare software development trends in 2026?
The eight leading trends are: ambient AI documentation moving to enterprise production, new CMS reimbursement codes making remote patient monitoring financially scalable, FHIR-native architecture as the default starting point for EHR-connected applications, a formal CPT billing structure for AI-augmented clinical decision support, behavioral health software as a standalone regulated category, legacy system modernization driven by cybersecurity and AI prerequisites, patient engagement software rebuilt around behavioral economics rather than information delivery, and cybersecurity treated as product architecture from day one. Each reflects the shift from piloting technologies to shipping production-grade systems with compliance and integration requirements built in from the start.
How is AI changing healthcare software development for U.S. product teams in 2026?
AI in 2026 has three primary application areas for U.S. product teams: ambient documentation integrated directly into clinical EHR workflows, clinical decision support tools backed by new CPT billing codes that enable formal reimbursement for AI-assisted services, and revenue cycle automation covering prior authorization, denial management, and claims optimization. CMS's January 2026 launch of the WISeR model — AI-supported prior authorization piloted in six states — signals the regulatory direction. Product teams are building explainability layers, audit trails, and mandatory clinician review workflows into AI features to manage the liability and compliance surface that clinical AI creates.
Why does FHIR matter for healthcare software product teams in 2026?
FHIR (Fast Healthcare Interoperability Resources) is the federal standard governing clinical data exchange, mandated by the 21st Century Cures Act's information blocking provisions. Any application connecting to major EHR platforms like Epic, Oracle Health, or athenahealth must be FHIR R4 compliant to participate in those ecosystems. SMART on FHIR is the specific OAuth 2.0 authorization framework those platforms use to authenticate third-party apps. Product teams that build FHIR-native from the architecture phase avoid significant rework, integration delays, and compliance gaps compared to teams that attempt to retrofit FHIR compatibility into an existing proprietary data model.
What did CMS change about remote patient monitoring reimbursement in 2026?
CMS's 2026 Physician Fee Schedule introduced CPT code 99445, which covers RPM device supply for patients who transmit physiologic data on 2–15 days in a 30-day period — previously, the only device supply code required a 16-day minimum. It also introduced CPT code 99470, which covers the first 10 minutes of treatment management services per month, down from the 20-minute minimum previously required under CPT 99457. These changes expand RPM eligibility to post-surgical recovery, episodic care, and patients with inconsistent monitoring adherence who were not reimbursable under prior rules, making RPM viable for a significantly larger patient population.
What does building a HIPAA-compliant healthcare app in 2026 actually require?
HIPAA technical safeguards in 2026 require zero-trust architecture across API connections, clinically aware role-based access controls, end-to-end encryption with documented key management, audit logging built into the data model (not added as an afterthought), documented patient consent workflows, and fully executed Business Associate Agreements with every third-party integration. Enterprise health system buyers now conduct detailed security architecture reviews before vendor selection, asking specifically how encryption, access control, and audit logging are implemented, not just whether a vendor claims HIPAA compliance. Security architecture documentation needs to be production-ready before the enterprise sales process begins.
Chinmay Chandgude


Chinmay Chandgude is a partner at Latent with over 9 years of experience in building custom digital platforms for healthcare and finance sectors. He focuses on creating scalable and secure web and mobile applications to drive technological transformation. Based in Pune, India, Chinmay is passionate about delivering user-centric solutions that improve efficiency and reduce costs.
Related Posts


Free Interactive Demo
Share your product idea — we'll design your MVP architecture for free, no commitment required. If it's a good fit, we'll show you what building it looks like.