Product Development

Chinmay Chandgude
Mobile Health Apps: Benefits, Features and What to Build in 2026

84 million Americans currently use healthcare apps. 65% say those apps have made managing their health easier. And yet hospital-provided app adoption in the US sits at roughly 2%.
That gap is not a demand problem. It is an execution problem.
The demand is there. The willingness to engage is there. What is missing is apps built around the things that actually improve health outcomes, not apps built around feature lists, market categories, or what was easiest to ship. Teams that understand what the evidence says about benefit, build features that deliver it, and design for the US payer and clinical context are the ones capturing that gap.
This article covers what the clinical research actually says about mobile health app benefits, which features are worth building to deliver them, and where the real US market opportunities sit in 2026.
Why the US mHealth Market Is Different from the Global Picture
The US mHealth apps market was valued at $14.44 billion in 2025 and is projected to reach $51.83 billion by 2034 at a 15.40% CAGR, the highest growth rate in North America, according to Precedence Research.
Globally, the mHealth apps market reached $40.65 billion in 2025 and is projected to grow to $113.2 billion by 2034 at an 11.80% CAGR according to Fortune Business Insights. North America holds 30.75% of that global market.
What makes the US market different is not just its size. It is the structural context: HIPAA, the 21st Century Cures Act's FHIR interoperability mandate, Medicare reimbursement for remote patient monitoring, and the FDA's Software as a Medical Device framework. These create real compliance requirements that raise build cost and timelines, but they also create a defensible moat for teams that get them right. A generic wellness app built for global markets cannot simply be repackaged for a US clinical environment.
Two US-specific numbers matter for anyone building in this space:
57% of US individuals used smartphone-based access to their medical records in 2024, a 50% rise in four years, according to the ASTP/ONC Health Information National Trends Survey (HINTS 7), the government's primary data source on this question. That is not a consumer trend. That is patients exercising rights created by the Cures Act, using apps to access records they are now legally entitled to.
The monitoring services segment holds 67.57% of the mHealth apps market in 2026 according to Fortune Business Insights, driven primarily by the aging population managing chronic conditions. The biggest segment in mHealth is not fitness. It is clinical monitoring. Teams building fitness and wellness apps are entering a crowded, lower-margin space. Teams building clinical monitoring tools are entering the segment with the most market, the most clinical evidence, and, for RPM, the most reimbursement infrastructure.
For context on the broader digital health picture, our guide to healthcare software development trends in 2026 covers how these market forces are reshaping what gets built.
The Proven Benefits of Mobile Health Apps: What the Evidence Actually Says
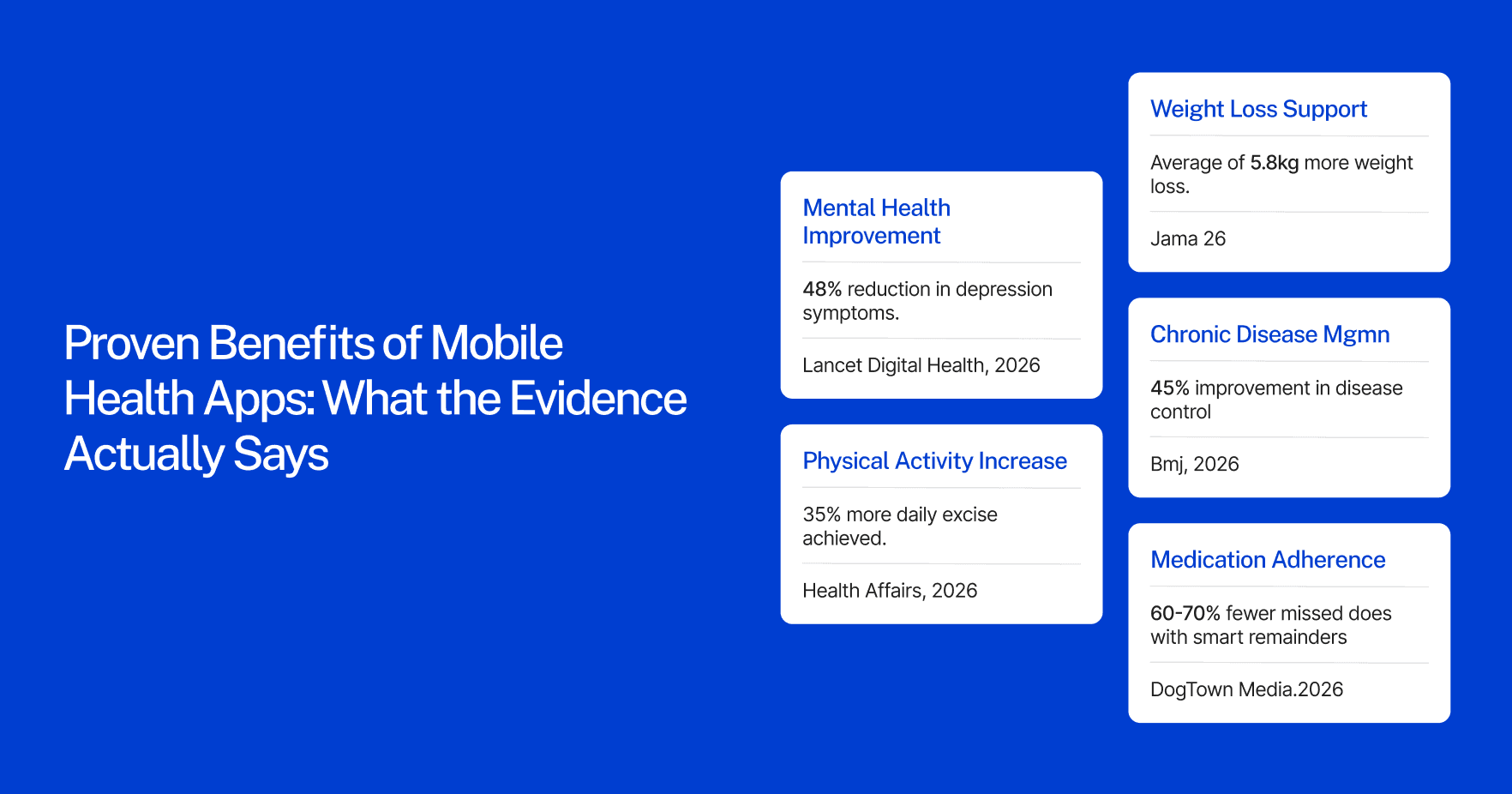
Most articles on this topic list benefits the same way a marketing deck lists features: accessibility, cost savings, patient engagement, better outcomes. The claims are real, but they float without evidence.
The evidence base for mHealth is now substantial. Over 2,000 studies on digital health app effectiveness have been published since 2007, with close to 1,500 in the past five years, according to the IQVIA Institute for Human Data Science Digital Health Trends 2021 report. Here is what the peer-reviewed literature actually supports, benefit by benefit.
Improved medication adherence in chronic disease management
Only 50% of chronically ill patients take medications as prescribed, leading to poor health outcomes, this is the finding that opens a 2025 systematic review and meta-analysis in the Journal of Medical Internet Research (JMIR), covering randomized controlled trials of mobile app interventions across patients with chronic conditions including hypertension, diabetes, and cardiovascular disease. The review, from McGill University's Department of Epidemiology, found that mobile apps produce consistent and moderate improvements in medication adherence across a diverse range of chronic conditions. Medication reminder features specifically reduce missed doses by 60–70% according to healthcare app development analysis by DogTown Media.
This is the benefit with the deepest RCT evidence base in mHealth. If you are evaluating whether a mobile app can improve clinical outcomes in chronic disease patients, the answer from the literature is yes, particularly for medication adherence, and particularly for apps that go beyond simple reminders to include personalized scheduling and provider-linked data.
Expanded care access, particularly in underserved US markets
Virtual visits cost 40–60% less than in-person appointments. That cost difference is not the main story, the access story is. For the 46 million Americans living in rural areas, for patients without reliable transportation, and for working adults who cannot take half a day off for a specialist visit, a telemedicine app is the difference between getting care and not getting care. The 57% smartphone-based medical records access figure from HINTS 7 reflects patients exercising a right, but it also reflects a usability shift: apps are increasingly the primary interface between patients and the healthcare system. For a deeper look at how that interface is built, see our guide to patient portal development.
Measurable reduction in hospital readmissions through remote monitoring
80% of US hospitals use wearables to support remote patient monitoring according to Grand View Research, citing industry data. Medicare's expansion of RPM billing codes has accelerated clinical adoption. Hospitals using RPM report 25–50% reductions in readmissions for chronic conditions including heart failure and diabetes, according to DogTown Media's healthcare app development analysis. The mechanism is simple: continuous data between visits catches deterioration before it becomes an emergency admission. Our guide to the benefits of wearable technology in healthcare covers how the device layer feeds these outcomes in practice.
Higher patient engagement with their own health data
65% of the US public say using health apps and websites has made managing their healthcare easier, according to KFF's Health Tracking Poll conducted in September 2025, a nationally representative survey of 1,334 US adults. This is a particularly strong finding because it comes from a US population survey, not a selected trial cohort. The result holds across age groups, including 45% of older Medicare enrollees who have used digital health tools in the past year.
Patient engagement with health data between visits is the mechanism behind almost every other benefit in this list. Patients who track, who see their own numbers, and who have a direct channel to their care team are more adherent, catch problems earlier, and have better long-term outcomes in chronic disease management.
Reduced administrative burden for providers
AI-powered ambient scribes integrated into clinical apps now save providers 2–3 hours daily on documentation according to DogTown Media. Apps that automate appointment scheduling, prescription refill requests, and care plan check-ins reduce the administrative overhead hitting care teams that are already operating at capacity. In a US healthcare system projecting a shortage of 86,000 physicians by 2036, every hour of documentation time saved is an hour of patient care restored.
For teams building products at the intersection of AI and care delivery, our guide to AI in healthcare product development in 2026 covers the specific architecture and compliance decisions involved.
Core Features That Deliver Those Benefits
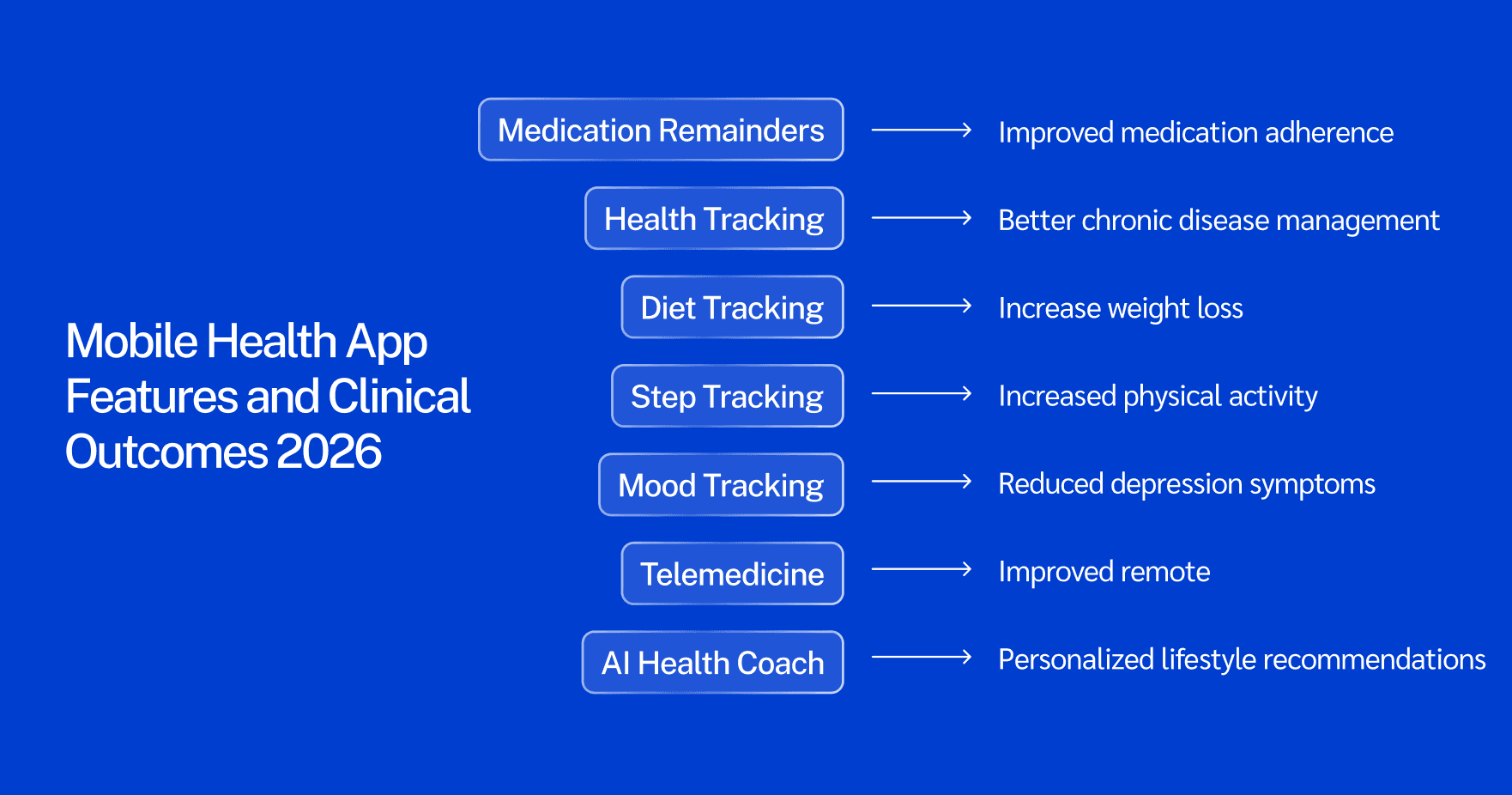
A 2026 mobile health app built for the US market needs five core feature categories: HIPAA-compliant data architecture, EHR integration via HL7/FHIR, wearable device connectivity, telemedicine with both async and video options, and medication management with smart reminders.
Features are not a checklist to complete. Each one maps to a clinical outcome. Teams that build feature lists without connecting them to an evidence-backed benefit end up building expensive apps that patients abandon within 30 days, and the data on this is stark. Only 3.4% of general health app users are still active by day 30.
The apps that retain users are the ones solving one specific clinical problem well. Chronic disease apps that connect medication reminders to wearable-tracked outcomes retain users at significantly higher rates than general wellness apps with 15 loosely related features. Teams building telemedicine as a core feature should review our telemedicine platform development guide before scoping the async and video infrastructure.
Feature | Clinical benefit delivered | Build complexity |
HIPAA-compliant data storage and messaging | Legal foundation; required for any US patient data | Medium (requires BAA-eligible cloud infrastructure) |
EHR/EMR integration (HL7/FHIR) | Continuous care record, clinical decision support | High (Epic, Cerner, and others vary significantly) |
Wearable device connectivity (Apple HealthKit, Google Fit, Samsung Health) | Remote monitoring, chronic disease tracking | Medium (SDK-based, device coverage varies) |
Smart medication reminders with personalized scheduling | 60–70% reduction in missed doses | Low to medium |
Async and video telemedicine | Cost reduction (40–60%), access expansion | High (real-time infrastructure, e-prescribing adds scope) |
Push notification engine with behavioral logic | Engagement, retention | Low |
AI-powered symptom checker or triage | First-response care, provider workload reduction | High (FDA SaMD considerations apply) |
Patient-facing health dashboard with trend visualization | Data engagement, early detection | Medium |
Provider-facing monitoring dashboard with alert logic | Readmission reduction, RPM billing | High |
On HIPAA: Compliance infrastructure is not a post-launch addition. HIPAA requirements consume 15–20% of a clinical app's total development budget when built from the start. Retrofitting them costs more and creates risk. Any app handling protected health information (PHI) in the US needs HIPAA-eligible cloud hosting, audit logs, role-based access controls, and a signed Business Associate Agreement with every vendor in the stack. Our guide to HIPAA-compliant app development covers what this means for architecture and vendor selection.
On FHIR: The 21st Century Cures Act requires certified health IT to support FHIR R4 APIs for patient data access. Apps that want to read or write EHR data, and most clinical apps do, need to build against this standard. This is the most technically complex feature category and the most consequential: the 57% of patients accessing records via smartphone apps are doing it through FHIR-enabled portals. Apps that ignore FHIR are building against the regulatory current. For implementation specifics, see our guide to FHIR integration for healthcare apps.
What Is Actually Worth Building in 2026: Four Validated US Market Opportunities
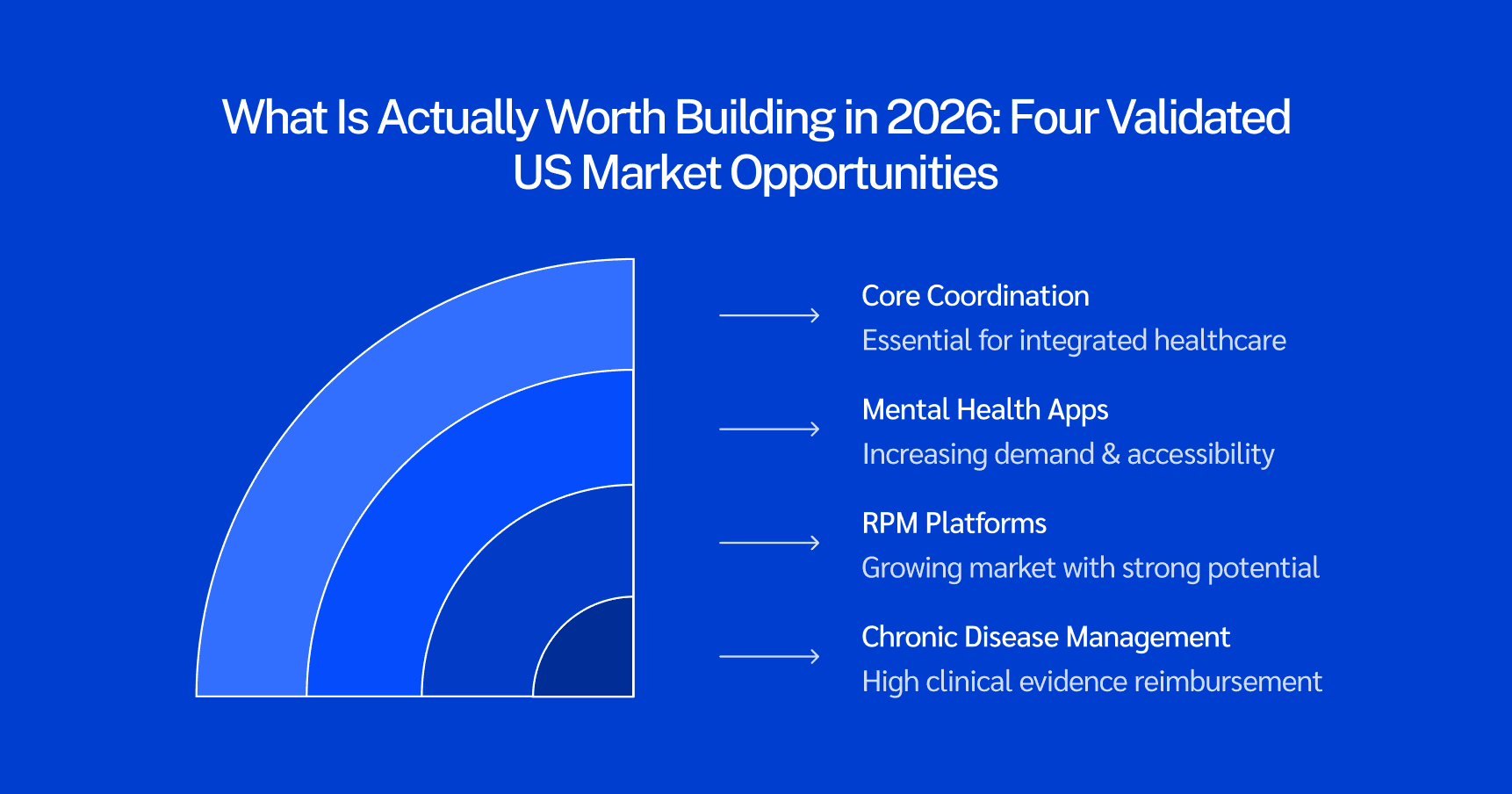
The US mHealth market has over 350,000 apps. Most of them are not successful. The apps that generate clinical value, and the revenue and reimbursement that follows from it, cluster in four categories with strong market and evidence support.
Chronic Disease Management Apps
Three in four American adults have at least one chronic condition, and over half have two or more, according to the CDC's chronic disease data. The clinical evidence base for mobile apps in chronic disease management is now the strongest in any mHealth category. The JMIR 2025 meta-analysis covers RCTs specifically for chronic condition medication adherence, making this the most evidence-supported build decision in mHealth.
Diabetes, hypertension, COPD, and cardiovascular disease are the priority areas. Each has a reimbursement pathway, an evidence base, and a large patient population. Build cost for a focused chronic disease management app with EHR integration typically runs $100,000–$250,000 depending on integration depth.
Remote Patient Monitoring Platforms
Medicare's CPT billing codes for RPM (99453, 99454, 99457, 99458) created a reimbursement pathway that most other mHealth categories lack. When an app is part of a billable clinical service, adoption becomes a financial decision for providers, not just a patient engagement experiment.
80% of US hospitals already use wearables for RPM. The software layer, apps that connect device data to provider workflows, generate alerts, and produce documentation for billing, is the build gap. RPM platforms need wearable connectivity, real-time alert logic, and provider-facing dashboards. Build cost runs $200,000–$400,000 for a platform handling multiple device types. For a breakdown of the device ecosystem these platforms need to integrate with, see our guide to top remote patient monitoring devices.
Mental Health and Behavioral Apps
Mental health apps are the fastest-growing category by user demand. The US has a shortfall of roughly one mental health provider per 350+ patients in many regions. Apps cannot replace providers, but they can extend the reach of the providers who exist, between-session support, mood tracking, CBT-based exercises, and crisis escalation pathways.
The regulatory split matters here. Wellness apps (stress reduction, meditation, mood tracking without clinical claims) require standard HIPAA compliance. Prescription digital therapeutics making clinical claims require FDA SaMD clearance, which adds 6–12 months and $200,000–$500,000 to the build. Teams need to make this call before they write a line of code. Our guide to Software as a Medical Device covers the classification decision and what it means for your development timeline.
Care Coordination for Underserved Populations
This is the highest-impact opportunity that the fewest teams execute well. 66% of large US hospital systems have patient apps available. Only 2% of their patients use them. The gap is not app availability, it is design.
Apps built for underserved populations need offline-first functionality for areas with poor connectivity, multilingual interfaces (Spanish is the minimum for any nationally distributed US health app), low-literacy design standards that communicate through visuals and simple language, and SMS-based notification fallbacks for patients without reliable smartphone data plans. These are not cosmetic changes, they are architecture decisions. Teams that treat them as cosmetic ship apps that sit unused in app stores.
Building in one of these categories? Latent has shipped healthcare products across 14 countries, with HIPAA compliance, sprint governance, and IP ownership built into the engagement from day one. Book a free discovery call and we will scope the right build for your situation.
What Makes a Mobile Health App Actually Succeed
Most mHealth apps fail to sustain engagement past 30 days. The apps that succeed share four build requirements that are decided before the first sprint, not discovered during post-launch troubleshooting.
Compliance architecture before features. HIPAA compliance built from the start costs 15–20% of total development budget. Retrofitted after launch, it costs substantially more and creates legal exposure during the gap. The same principle applies to FDA SaMD classification: if an app will make diagnostic or treatment claims, the regulatory pathway needs to be scoped before architecture decisions are made, not after product-market fit is found.
Genuine EHR interoperability, not a workaround. FHIR R4 is the current interoperability standard under the Cures Act. An app that pulls data from Apple Health or a proprietary wearable without connecting to the clinical record is building a parallel data silo. Patients and providers increasingly expect the app to talk to the EHR. Apps that cannot do this are losing ground in clinical adoption.
Feature prioritization by outcome, not by scope. The RCT evidence is clear: apps with one focused clinical function retain users and change behavior. Apps with 15 loosely connected features do not. The product question at every sprint is not "what else can we add?" It is "does this feature produce the clinical outcome we are building toward?"
Build for the payer logic. RPM is reimbursable. Some digital therapeutics are covered by commercial insurers. Chronic disease management programs tied to value-based care contracts are fundable. Apps that map their feature set to CPT codes and value-based metrics become part of clinical workflows, and get adopted at rates that consumer-only apps cannot match.
Teams evaluating whether to build in-house or with an outside partner will find the decision framework in our guide to outsourcing healthcare product development. For the technical build process itself, our guide to how to develop a healthcare app walks through the full development lifecycle from discovery to deployment.
How Much Does It Cost to Build a Mobile Health App in 2026?
Building a mobile health app in 2026 typically costs $50,000–$150,000 for a focused MVP, $150,000–$300,000 for a mid-tier clinical platform with EHR integration, and $300,000+ for an enterprise system with full HIPAA, AI, and multi-EHR support.
App type | Typical build range | Key cost drivers |
Wellness or fitness app (no PHI, no EHR) | $50,000–$80,000 | UX, wearable SDK, notification logic |
Patient-facing clinical app with portal access | $100,000–$200,000 | FHIR integration, HIPAA infra, compliance review |
Telemedicine platform | $150,000–$300,000 | Real-time video, async messaging, e-prescribing |
Remote patient monitoring platform | $200,000–$400,000 | Device connectivity, alert logic, provider dashboard |
Enterprise clinical platform | $300,000–$500,000+ | Multi-EHR, AI features, FDA SaMD path |
Three costs that most budget estimates miss:
HIPAA compliance infrastructure adds $10,000–$20,000 to any app handling protected health information. Annual maintenance runs 15–25% of the initial build cost, security patches, OS updates, new device SDK versions, and ongoing compliance reviews are not optional for clinical apps. And EHR integration scope varies significantly by the EHR system: Epic and Cerner each have their own FHIR implementation details, API documentation, and sandbox approval processes that affect timeline by weeks.
For teams building clinical products, the managed pod model delivers the compliance-ready infrastructure from sprint one, architecture decisions, PHI handling, and sprint compliance logs are default outputs rather than post-launch retrofits. Latent's managed pods typically deliver healthcare MVPs in 8–14 weeks for focused scopes, with IP ownership, HIPAA documentation, and sprint visibility included in the engagement structure.
For a deeper look at how engagement models affect build cost and accountability, see our guide to what is a managed development team. And if you are starting from an idea with no existing codebase, our guide to launching your first healthtech app in under 90 days maps the fastest compliant path from concept to live product. For full cost benchmarks and budget breakdown templates, see our dedicated healthcare app development cost guide.
Build the App That Closes the Gap
The 84 million Americans already using health apps are not waiting for a new feature. They are waiting for an app that solves a real clinical problem, works with their existing care, and gives them a reason to come back.
The evidence points to where that gap is: chronic disease patients who miss half their doses, rural patients without specialist access, hospital systems with monitoring infrastructure but no software layer that ties it to outcomes, and care coordination for the patients most underserved by the current system.
The teams that close this gap are not the ones with the largest feature roadmaps. They are the ones who started with a specific clinical problem, cited the evidence, built the feature that addresses it, and shipped with HIPAA and interoperability handled from the start.
Latent builds healthcare products using managed execution pods, cross-functional teams that own delivery from sprint planning through deployment, with HIPAA compliance, FHIR architecture, and IP documentation built into the operating rhythm. We have shipped 100+ products across 14 countries, including clinical apps, RPM platforms, telemedicine tools, and patient engagement systems.
If you are evaluating a mobile health app build, whether that is a focused MVP to test a clinical hypothesis or a full clinical platform, book a free 30-minute discovery call. We will scope the architecture, map the compliance decisions, and give you a realistic build estimate before you commit to anything.
Or start with a free 2-week discovery sprint: we scope the clinical use case, define the compliance path, and produce the architecture before your first dollar of development spend. Book your free discovery sprint.
Frequently Asked Questions
What are the benefits of mobile health apps?
The five most evidence-supported benefits of mobile health apps are: improved medication adherence in chronic disease patients (consistent moderate improvements across RCTs per JMIR 2025 meta-analysis), expanded care access through virtual visits at 40–60% lower cost than in-person appointments, reduced hospital readmissions through remote patient monitoring (25–50% reduction for heart failure and diabetes), higher patient engagement with their own health data (65% of US adults say apps made managing health easier per KFF 2025), and reduced provider administrative burden through AI-assisted documentation and automated workflows.
How much does it cost to build a mobile health app in 2026?
Building a mobile health app in 2026 typically costs $50,000–$80,000 for a wellness app with no clinical data, $100,000–$200,000 for a patient-facing clinical app with EHR access, $150,000–$300,000 for a telemedicine platform, and $200,000–$400,000 for a remote patient monitoring platform with device connectivity and provider dashboards. HIPAA compliance infrastructure adds $10,000–$20,000 to any app handling protected health information, and annual maintenance runs 15–25% of initial build cost.
What features should a mobile health app have?
A 2026 US-market mHealth app needs five core feature categories: HIPAA-compliant data storage and messaging (required for any app handling patient data), EHR/EMR integration using HL7/FHIR standards, wearable device connectivity via Apple HealthKit or Google Fit, medication management with smart reminders, and telemedicine with async and video options. The specific feature set depends on the clinical use case, a chronic disease management app and a telemedicine platform have different priority features even though both serve patient health.
What types of mobile health apps are most successful in the US in 2026?
The four mHealth categories with the strongest US market evidence in 2026 are: chronic disease management apps (strongest clinical evidence base from RCTs, largest patient population), remote patient monitoring platforms (Medicare-reimbursable via RPM billing codes, 80% US hospital infrastructure already in place), mental health and behavioral apps (fastest-growing user demand, large provider shortage to address), and care coordination tools for underserved populations (highest unmet need, 98% of patients at large US hospitals not using available hospital apps).
What regulations apply to mobile health apps in the US?
US mobile health apps face three primary regulatory frameworks. HIPAA applies to any app handling protected health information, it governs data storage, transmission, access controls, and vendor agreements. The FDA's Software as a Medical Device (SaMD) framework applies to apps making diagnostic or treatment claims; these require FDA clearance before market release. The 21st Century Cures Act requires FHIR R4 API support for certified health IT and gives patients the right to access their records via third-party apps, any clinical app expecting EHR access needs to build against this standard. Wellness apps making no clinical claims have lower regulatory overhead but still require HIPAA compliance if they collect personally identifiable health data.
84 million Americans currently use healthcare apps. 65% say those apps have made managing their health easier. And yet hospital-provided app adoption in the US sits at roughly 2%.
That gap is not a demand problem. It is an execution problem.
The demand is there. The willingness to engage is there. What is missing is apps built around the things that actually improve health outcomes, not apps built around feature lists, market categories, or what was easiest to ship. Teams that understand what the evidence says about benefit, build features that deliver it, and design for the US payer and clinical context are the ones capturing that gap.
This article covers what the clinical research actually says about mobile health app benefits, which features are worth building to deliver them, and where the real US market opportunities sit in 2026.
Why the US mHealth Market Is Different from the Global Picture
The US mHealth apps market was valued at $14.44 billion in 2025 and is projected to reach $51.83 billion by 2034 at a 15.40% CAGR, the highest growth rate in North America, according to Precedence Research.
Globally, the mHealth apps market reached $40.65 billion in 2025 and is projected to grow to $113.2 billion by 2034 at an 11.80% CAGR according to Fortune Business Insights. North America holds 30.75% of that global market.
What makes the US market different is not just its size. It is the structural context: HIPAA, the 21st Century Cures Act's FHIR interoperability mandate, Medicare reimbursement for remote patient monitoring, and the FDA's Software as a Medical Device framework. These create real compliance requirements that raise build cost and timelines, but they also create a defensible moat for teams that get them right. A generic wellness app built for global markets cannot simply be repackaged for a US clinical environment.
Two US-specific numbers matter for anyone building in this space:
57% of US individuals used smartphone-based access to their medical records in 2024, a 50% rise in four years, according to the ASTP/ONC Health Information National Trends Survey (HINTS 7), the government's primary data source on this question. That is not a consumer trend. That is patients exercising rights created by the Cures Act, using apps to access records they are now legally entitled to.
The monitoring services segment holds 67.57% of the mHealth apps market in 2026 according to Fortune Business Insights, driven primarily by the aging population managing chronic conditions. The biggest segment in mHealth is not fitness. It is clinical monitoring. Teams building fitness and wellness apps are entering a crowded, lower-margin space. Teams building clinical monitoring tools are entering the segment with the most market, the most clinical evidence, and, for RPM, the most reimbursement infrastructure.
For context on the broader digital health picture, our guide to healthcare software development trends in 2026 covers how these market forces are reshaping what gets built.
The Proven Benefits of Mobile Health Apps: What the Evidence Actually Says
Most articles on this topic list benefits the same way a marketing deck lists features: accessibility, cost savings, patient engagement, better outcomes. The claims are real, but they float without evidence.
The evidence base for mHealth is now substantial. Over 2,000 studies on digital health app effectiveness have been published since 2007, with close to 1,500 in the past five years, according to the IQVIA Institute for Human Data Science Digital Health Trends 2021 report. Here is what the peer-reviewed literature actually supports, benefit by benefit.
Improved medication adherence in chronic disease management
Only 50% of chronically ill patients take medications as prescribed, leading to poor health outcomes, this is the finding that opens a 2025 systematic review and meta-analysis in the Journal of Medical Internet Research (JMIR), covering randomized controlled trials of mobile app interventions across patients with chronic conditions including hypertension, diabetes, and cardiovascular disease. The review, from McGill University's Department of Epidemiology, found that mobile apps produce consistent and moderate improvements in medication adherence across a diverse range of chronic conditions. Medication reminder features specifically reduce missed doses by 60–70% according to healthcare app development analysis by DogTown Media.
This is the benefit with the deepest RCT evidence base in mHealth. If you are evaluating whether a mobile app can improve clinical outcomes in chronic disease patients, the answer from the literature is yes, particularly for medication adherence, and particularly for apps that go beyond simple reminders to include personalized scheduling and provider-linked data.
Expanded care access, particularly in underserved US markets
Virtual visits cost 40–60% less than in-person appointments. That cost difference is not the main story, the access story is. For the 46 million Americans living in rural areas, for patients without reliable transportation, and for working adults who cannot take half a day off for a specialist visit, a telemedicine app is the difference between getting care and not getting care. The 57% smartphone-based medical records access figure from HINTS 7 reflects patients exercising a right, but it also reflects a usability shift: apps are increasingly the primary interface between patients and the healthcare system. For a deeper look at how that interface is built, see our guide to patient portal development.
Measurable reduction in hospital readmissions through remote monitoring
80% of US hospitals use wearables to support remote patient monitoring according to Grand View Research, citing industry data. Medicare's expansion of RPM billing codes has accelerated clinical adoption. Hospitals using RPM report 25–50% reductions in readmissions for chronic conditions including heart failure and diabetes, according to DogTown Media's healthcare app development analysis. The mechanism is simple: continuous data between visits catches deterioration before it becomes an emergency admission. Our guide to the benefits of wearable technology in healthcare covers how the device layer feeds these outcomes in practice.
Higher patient engagement with their own health data
65% of the US public say using health apps and websites has made managing their healthcare easier, according to KFF's Health Tracking Poll conducted in September 2025, a nationally representative survey of 1,334 US adults. This is a particularly strong finding because it comes from a US population survey, not a selected trial cohort. The result holds across age groups, including 45% of older Medicare enrollees who have used digital health tools in the past year.
Patient engagement with health data between visits is the mechanism behind almost every other benefit in this list. Patients who track, who see their own numbers, and who have a direct channel to their care team are more adherent, catch problems earlier, and have better long-term outcomes in chronic disease management.
Reduced administrative burden for providers
AI-powered ambient scribes integrated into clinical apps now save providers 2–3 hours daily on documentation according to DogTown Media. Apps that automate appointment scheduling, prescription refill requests, and care plan check-ins reduce the administrative overhead hitting care teams that are already operating at capacity. In a US healthcare system projecting a shortage of 86,000 physicians by 2036, every hour of documentation time saved is an hour of patient care restored.
For teams building products at the intersection of AI and care delivery, our guide to AI in healthcare product development in 2026 covers the specific architecture and compliance decisions involved.
Core Features That Deliver Those Benefits
A 2026 mobile health app built for the US market needs five core feature categories: HIPAA-compliant data architecture, EHR integration via HL7/FHIR, wearable device connectivity, telemedicine with both async and video options, and medication management with smart reminders.
Features are not a checklist to complete. Each one maps to a clinical outcome. Teams that build feature lists without connecting them to an evidence-backed benefit end up building expensive apps that patients abandon within 30 days, and the data on this is stark. Only 3.4% of general health app users are still active by day 30.
The apps that retain users are the ones solving one specific clinical problem well. Chronic disease apps that connect medication reminders to wearable-tracked outcomes retain users at significantly higher rates than general wellness apps with 15 loosely related features. Teams building telemedicine as a core feature should review our telemedicine platform development guide before scoping the async and video infrastructure.
Feature | Clinical benefit delivered | Build complexity |
HIPAA-compliant data storage and messaging | Legal foundation; required for any US patient data | Medium (requires BAA-eligible cloud infrastructure) |
EHR/EMR integration (HL7/FHIR) | Continuous care record, clinical decision support | High (Epic, Cerner, and others vary significantly) |
Wearable device connectivity (Apple HealthKit, Google Fit, Samsung Health) | Remote monitoring, chronic disease tracking | Medium (SDK-based, device coverage varies) |
Smart medication reminders with personalized scheduling | 60–70% reduction in missed doses | Low to medium |
Async and video telemedicine | Cost reduction (40–60%), access expansion | High (real-time infrastructure, e-prescribing adds scope) |
Push notification engine with behavioral logic | Engagement, retention | Low |
AI-powered symptom checker or triage | First-response care, provider workload reduction | High (FDA SaMD considerations apply) |
Patient-facing health dashboard with trend visualization | Data engagement, early detection | Medium |
Provider-facing monitoring dashboard with alert logic | Readmission reduction, RPM billing | High |
On HIPAA: Compliance infrastructure is not a post-launch addition. HIPAA requirements consume 15–20% of a clinical app's total development budget when built from the start. Retrofitting them costs more and creates risk. Any app handling protected health information (PHI) in the US needs HIPAA-eligible cloud hosting, audit logs, role-based access controls, and a signed Business Associate Agreement with every vendor in the stack. Our guide to HIPAA-compliant app development covers what this means for architecture and vendor selection.
On FHIR: The 21st Century Cures Act requires certified health IT to support FHIR R4 APIs for patient data access. Apps that want to read or write EHR data, and most clinical apps do, need to build against this standard. This is the most technically complex feature category and the most consequential: the 57% of patients accessing records via smartphone apps are doing it through FHIR-enabled portals. Apps that ignore FHIR are building against the regulatory current. For implementation specifics, see our guide to FHIR integration for healthcare apps.
What Is Actually Worth Building in 2026: Four Validated US Market Opportunities
The US mHealth market has over 350,000 apps. Most of them are not successful. The apps that generate clinical value, and the revenue and reimbursement that follows from it, cluster in four categories with strong market and evidence support.
Chronic Disease Management Apps
Three in four American adults have at least one chronic condition, and over half have two or more, according to the CDC's chronic disease data. The clinical evidence base for mobile apps in chronic disease management is now the strongest in any mHealth category. The JMIR 2025 meta-analysis covers RCTs specifically for chronic condition medication adherence, making this the most evidence-supported build decision in mHealth.
Diabetes, hypertension, COPD, and cardiovascular disease are the priority areas. Each has a reimbursement pathway, an evidence base, and a large patient population. Build cost for a focused chronic disease management app with EHR integration typically runs $100,000–$250,000 depending on integration depth.
Remote Patient Monitoring Platforms
Medicare's CPT billing codes for RPM (99453, 99454, 99457, 99458) created a reimbursement pathway that most other mHealth categories lack. When an app is part of a billable clinical service, adoption becomes a financial decision for providers, not just a patient engagement experiment.
80% of US hospitals already use wearables for RPM. The software layer, apps that connect device data to provider workflows, generate alerts, and produce documentation for billing, is the build gap. RPM platforms need wearable connectivity, real-time alert logic, and provider-facing dashboards. Build cost runs $200,000–$400,000 for a platform handling multiple device types. For a breakdown of the device ecosystem these platforms need to integrate with, see our guide to top remote patient monitoring devices.
Mental Health and Behavioral Apps
Mental health apps are the fastest-growing category by user demand. The US has a shortfall of roughly one mental health provider per 350+ patients in many regions. Apps cannot replace providers, but they can extend the reach of the providers who exist, between-session support, mood tracking, CBT-based exercises, and crisis escalation pathways.
The regulatory split matters here. Wellness apps (stress reduction, meditation, mood tracking without clinical claims) require standard HIPAA compliance. Prescription digital therapeutics making clinical claims require FDA SaMD clearance, which adds 6–12 months and $200,000–$500,000 to the build. Teams need to make this call before they write a line of code. Our guide to Software as a Medical Device covers the classification decision and what it means for your development timeline.
Care Coordination for Underserved Populations
This is the highest-impact opportunity that the fewest teams execute well. 66% of large US hospital systems have patient apps available. Only 2% of their patients use them. The gap is not app availability, it is design.
Apps built for underserved populations need offline-first functionality for areas with poor connectivity, multilingual interfaces (Spanish is the minimum for any nationally distributed US health app), low-literacy design standards that communicate through visuals and simple language, and SMS-based notification fallbacks for patients without reliable smartphone data plans. These are not cosmetic changes, they are architecture decisions. Teams that treat them as cosmetic ship apps that sit unused in app stores.
Building in one of these categories? Latent has shipped healthcare products across 14 countries, with HIPAA compliance, sprint governance, and IP ownership built into the engagement from day one. Book a free discovery call and we will scope the right build for your situation.
What Makes a Mobile Health App Actually Succeed
Most mHealth apps fail to sustain engagement past 30 days. The apps that succeed share four build requirements that are decided before the first sprint, not discovered during post-launch troubleshooting.
Compliance architecture before features. HIPAA compliance built from the start costs 15–20% of total development budget. Retrofitted after launch, it costs substantially more and creates legal exposure during the gap. The same principle applies to FDA SaMD classification: if an app will make diagnostic or treatment claims, the regulatory pathway needs to be scoped before architecture decisions are made, not after product-market fit is found.
Genuine EHR interoperability, not a workaround. FHIR R4 is the current interoperability standard under the Cures Act. An app that pulls data from Apple Health or a proprietary wearable without connecting to the clinical record is building a parallel data silo. Patients and providers increasingly expect the app to talk to the EHR. Apps that cannot do this are losing ground in clinical adoption.
Feature prioritization by outcome, not by scope. The RCT evidence is clear: apps with one focused clinical function retain users and change behavior. Apps with 15 loosely connected features do not. The product question at every sprint is not "what else can we add?" It is "does this feature produce the clinical outcome we are building toward?"
Build for the payer logic. RPM is reimbursable. Some digital therapeutics are covered by commercial insurers. Chronic disease management programs tied to value-based care contracts are fundable. Apps that map their feature set to CPT codes and value-based metrics become part of clinical workflows, and get adopted at rates that consumer-only apps cannot match.
Teams evaluating whether to build in-house or with an outside partner will find the decision framework in our guide to outsourcing healthcare product development. For the technical build process itself, our guide to how to develop a healthcare app walks through the full development lifecycle from discovery to deployment.
How Much Does It Cost to Build a Mobile Health App in 2026?
Building a mobile health app in 2026 typically costs $50,000–$150,000 for a focused MVP, $150,000–$300,000 for a mid-tier clinical platform with EHR integration, and $300,000+ for an enterprise system with full HIPAA, AI, and multi-EHR support.
App type | Typical build range | Key cost drivers |
Wellness or fitness app (no PHI, no EHR) | $50,000–$80,000 | UX, wearable SDK, notification logic |
Patient-facing clinical app with portal access | $100,000–$200,000 | FHIR integration, HIPAA infra, compliance review |
Telemedicine platform | $150,000–$300,000 | Real-time video, async messaging, e-prescribing |
Remote patient monitoring platform | $200,000–$400,000 | Device connectivity, alert logic, provider dashboard |
Enterprise clinical platform | $300,000–$500,000+ | Multi-EHR, AI features, FDA SaMD path |
Three costs that most budget estimates miss:
HIPAA compliance infrastructure adds $10,000–$20,000 to any app handling protected health information. Annual maintenance runs 15–25% of the initial build cost, security patches, OS updates, new device SDK versions, and ongoing compliance reviews are not optional for clinical apps. And EHR integration scope varies significantly by the EHR system: Epic and Cerner each have their own FHIR implementation details, API documentation, and sandbox approval processes that affect timeline by weeks.
For teams building clinical products, the managed pod model delivers the compliance-ready infrastructure from sprint one, architecture decisions, PHI handling, and sprint compliance logs are default outputs rather than post-launch retrofits. Latent's managed pods typically deliver healthcare MVPs in 8–14 weeks for focused scopes, with IP ownership, HIPAA documentation, and sprint visibility included in the engagement structure.
For a deeper look at how engagement models affect build cost and accountability, see our guide to what is a managed development team. And if you are starting from an idea with no existing codebase, our guide to launching your first healthtech app in under 90 days maps the fastest compliant path from concept to live product. For full cost benchmarks and budget breakdown templates, see our dedicated healthcare app development cost guide.
Build the App That Closes the Gap
The 84 million Americans already using health apps are not waiting for a new feature. They are waiting for an app that solves a real clinical problem, works with their existing care, and gives them a reason to come back.
The evidence points to where that gap is: chronic disease patients who miss half their doses, rural patients without specialist access, hospital systems with monitoring infrastructure but no software layer that ties it to outcomes, and care coordination for the patients most underserved by the current system.
The teams that close this gap are not the ones with the largest feature roadmaps. They are the ones who started with a specific clinical problem, cited the evidence, built the feature that addresses it, and shipped with HIPAA and interoperability handled from the start.
Latent builds healthcare products using managed execution pods, cross-functional teams that own delivery from sprint planning through deployment, with HIPAA compliance, FHIR architecture, and IP documentation built into the operating rhythm. We have shipped 100+ products across 14 countries, including clinical apps, RPM platforms, telemedicine tools, and patient engagement systems.
If you are evaluating a mobile health app build, whether that is a focused MVP to test a clinical hypothesis or a full clinical platform, book a free 30-minute discovery call. We will scope the architecture, map the compliance decisions, and give you a realistic build estimate before you commit to anything.
Or start with a free 2-week discovery sprint: we scope the clinical use case, define the compliance path, and produce the architecture before your first dollar of development spend. Book your free discovery sprint.
Frequently Asked Questions
What are the benefits of mobile health apps?
The five most evidence-supported benefits of mobile health apps are: improved medication adherence in chronic disease patients (consistent moderate improvements across RCTs per JMIR 2025 meta-analysis), expanded care access through virtual visits at 40–60% lower cost than in-person appointments, reduced hospital readmissions through remote patient monitoring (25–50% reduction for heart failure and diabetes), higher patient engagement with their own health data (65% of US adults say apps made managing health easier per KFF 2025), and reduced provider administrative burden through AI-assisted documentation and automated workflows.
How much does it cost to build a mobile health app in 2026?
Building a mobile health app in 2026 typically costs $50,000–$80,000 for a wellness app with no clinical data, $100,000–$200,000 for a patient-facing clinical app with EHR access, $150,000–$300,000 for a telemedicine platform, and $200,000–$400,000 for a remote patient monitoring platform with device connectivity and provider dashboards. HIPAA compliance infrastructure adds $10,000–$20,000 to any app handling protected health information, and annual maintenance runs 15–25% of initial build cost.
What features should a mobile health app have?
A 2026 US-market mHealth app needs five core feature categories: HIPAA-compliant data storage and messaging (required for any app handling patient data), EHR/EMR integration using HL7/FHIR standards, wearable device connectivity via Apple HealthKit or Google Fit, medication management with smart reminders, and telemedicine with async and video options. The specific feature set depends on the clinical use case, a chronic disease management app and a telemedicine platform have different priority features even though both serve patient health.
What types of mobile health apps are most successful in the US in 2026?
The four mHealth categories with the strongest US market evidence in 2026 are: chronic disease management apps (strongest clinical evidence base from RCTs, largest patient population), remote patient monitoring platforms (Medicare-reimbursable via RPM billing codes, 80% US hospital infrastructure already in place), mental health and behavioral apps (fastest-growing user demand, large provider shortage to address), and care coordination tools for underserved populations (highest unmet need, 98% of patients at large US hospitals not using available hospital apps).
What regulations apply to mobile health apps in the US?
US mobile health apps face three primary regulatory frameworks. HIPAA applies to any app handling protected health information, it governs data storage, transmission, access controls, and vendor agreements. The FDA's Software as a Medical Device (SaMD) framework applies to apps making diagnostic or treatment claims; these require FDA clearance before market release. The 21st Century Cures Act requires FHIR R4 API support for certified health IT and gives patients the right to access their records via third-party apps, any clinical app expecting EHR access needs to build against this standard. Wellness apps making no clinical claims have lower regulatory overhead but still require HIPAA compliance if they collect personally identifiable health data.
Chinmay Chandgude


Chinmay Chandgude is a partner at Latent with over 9 years of experience in building custom digital platforms for healthcare and finance sectors. He focuses on creating scalable and secure web and mobile applications to drive technological transformation. Based in Pune, India, Chinmay is passionate about delivering user-centric solutions that improve efficiency and reduce costs.
Related Posts


Free Interactive Demo
Share your product idea — we'll design your MVP architecture for free, no commitment required. If it's a good fit, we'll show you what building it looks like.